Thyrotoxicosis Associated Channelopathy
<p>We hereby report a case of 47 year-old man of Indian origin whose hyperthyroidism surfaced when he presented with an episode of muscular paralysis in association with hypokalemia. Weakness recovered with the correction of hypokalemia and the thyroid activity. Thyrotoxic Periodic Paralysis (TPP) is a rare life threatening complication of hyperthyroidism. Awareness of the entity not only helps in definitive treatment of the disease but also aids in timely detection of primary pathology. Recent advances in the understanding of the pathogenesis are been discussed.</p>
Introduction
TPP is characterized by a triad of episodes of muscle weakness and hypokalemia in a patient of thyrotoxicosis. Latter, though essential, can be subtle and of any etiology, including fictitious thyrotoxicosis [1]. It is more common in East Asian men - 1.8% in Chinese versus 0.1%-0.2% in North Americans [1]. Male to female ratio ranges from 17:1 to 70:1 [1]. It is often confused with Familial Periodic Paralysis (FPP) as the neuromuscular presentations of the two are very similar and the features of thyrotoxicosis may be subtle. Weakness usually starts in the lower limbs; often, after taking a heavy meal or alcohol. Rest after a physical exercise can also initiate the paralysis. Correct diagnosis helps institute a definitive treatment and avoids the risk of rebound hyperkalemia, which was seen in 59% of patients treated with potassium supplement [2, 3].
Association of TPP with HLA-DRw8 suggests a genetic predisposition and the 17q24.3 locus had been linked to it [4].
A 47 years old man of Indian origin, journalist by occupation, presented with acute onset of weakness of all 4 limbs for 1 day. One day earlier, when the patient woke up in the morning, he was not able to rise from the bed. Weakness did not fluctuate or progress further. All four limbs were weak, proximally as well as distally but the sensations were intact. He was able to pass urine and stools. There was no preceding history of infection, diarrhea or vaccination. There was no prior history of exercise or carbohydrate rich food. There was no history of drooping of eye lids, double vision, and difficulty in swallowing or speaking. He did not have pain in abdomen or dark colored urine. On further questioning, patient confirmed preceding history of palpitation, weight loss and heat intolerance. Patient had similar weakness 8 months back for which he took treatment from local hospital and became better. No one in the family had similar disease and he did not take any drugs or medicines. He did not have diabetes mellitus, hypertension or tuberculosis. He was non-smoker and non-alcoholic. His diet was mixed and he had normal appetite and sleep. Patient was conscious and cooperative. He was of average built and height with a BMI of 19 kg/m2. His resting pulse rate was 116/minute and other vital signs were normal. His general examination was normal except that he had fine tremors. There was diffuse thyroid swelling about 4 cm x2 cm in size in the neck. It was non tender and firm and was moving with deglutition. Bruit was not audible over it. Lymphnodes or nodules were not palpable in the neck. On neurological examination, his higher functions and cranial nerves were normal. With support he was able to sit and could hold his neck. There were no signs of meningeal irritation. Tone of muscles of all the limbs was reduced and power was of grade 2/5. Deep tendon jerks were intact. Sensory and cerebellar functions, as far as could be tested, were normal. Other organ systems were also normal. His routine laboratory tests including CBC, Plasma glucose level, LFT, KFT and lipid profile were normal. Levels of serum sodium, potassium and chloride were 137.9 mmol/l (reference range 135-145), 2.87 mmol/l (ref. range 3.6-5.5) and 106.9 mmol/l (ref. range 97-107), respectively. His Serum TSH level (done by CLIA method) was 0.01 µIU/ml (ref. range 0.35-5.50), Serum T3 was >8.0 ng/ml (ref. range 0.60 to 1.81) and serum T4 was >30 µgm/dl (ref. range 5.01-12.45). ECG showed sinus tachycardia. USG Neck showed both lobes of thyroid gland enlarged and bulky and of heterogenous echo-texture. No nodule was identified. Color Doppler showed increased vascularity. Significant lymphadenopathy was not seen. Patient was given potassium chloride, Propranolol and carbimazole. Patient regained muscle power within a day and his serum potassium level became 4.87mmol/l. After eight months of this episode, patient is euthyroid and is keeping well on carbimazole without any episode of the weakness.
Discussion
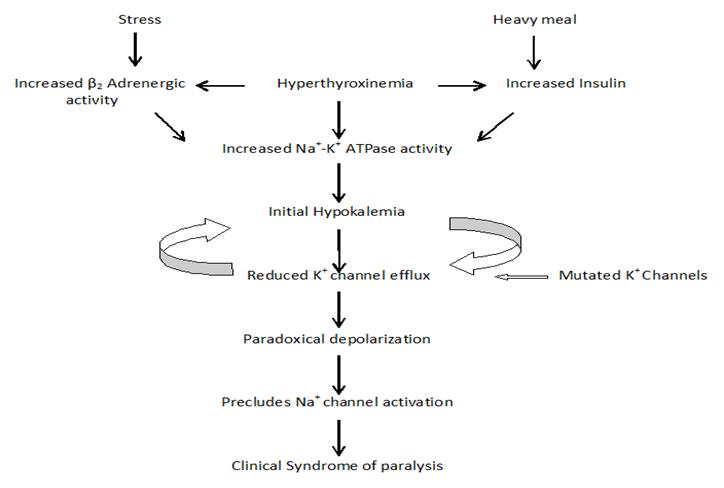
Diagnosis of TPP is based on clinical and biochemical evidence of episodic flaccid muscle weakness and hypokalemia in a patient of thyrotoxicosis. Cognitive and sensory deficit are not seen. Family history of periodic paralysis is exceptional [5]. Tests could not be performed to show the presence of specific anticorps in our patient, nevertheless, based on cumulative clinical and sonography parameters, it fits well in Graves’ disease. As such, any source of elevated thyroxin, including exogenous and TSH secreting tumors can cause the syndrome of TPP [1]. Extracellular potassium level is crucial to maintain action potential of sarcolemma [6]. In TPP, hypokalemia is due to shift of potassium from extracellular space to intracellular space and there is no net loss from the body [3]. Extracellular potassium homeostasis is mediated by specific transporters and channels in the cell membrane of the body tissues. Ingress of the ion into the cell is by ubiquitous Na+K+-ATPase and the egress is by inward- rectifier K+ (Kir) channel, as also by voltage-gated K+ (Kv) channel [6]. Kir channels allow rectification by unequal movement of potassium to and from the cell [6]. Kir2.6 channel, one of the 7 subfamilies of Kir channels is exclusively found in skeletal muscles [3]. Transport of the K+ ion is modified by the carbohydrate rich meal and thus insulin level, physical activity, adrenergic tone, hormones, drugs, poisons and the mutations in the genes encoding the channels [1]. This explains the fluctuating nature of weakness seen in the channelopathies [7].
Recently, mutation of the KCNJ2 gene, encoding the inward-rectifier potassium channel (Kir2.6) has been found in upto 33% of cases [5]. In others, it could be explained by polymorphism or mutations in the non coding introns [4]. A genetic variant (TC genotype) is located in the long intergenic non-coding RNA (linkRNA) downstream of Kir channel genes [4]. Variation in expression of linkRNA and Kir Channel correlates with the serum thyroxin level and TC genotype [4]. Thyroid hormone increases mRNA and thus proteins for the α-subunit of the Na+K+-ATPase leading to the abundance of the transporter [1]. Thyroid responsive elements are also found in the promoter region of the gene encoding the Kir2.6 channel [1]. Loss of function mutation of the gene for Kir2.6 channel down regulates its function. This, coupled with increased expression/abundance of Na+K+-ATPase can explain the role of thyroxin in causing hypokalemia during thyrotoxicosis and correcting it in euthyroid state. β- adrenergic activity is increased during thyrotoxicosis which in turn amplifies the activity of the Na+K+-ATPase. This explains the therapeutic role of nonselective β- blockers in TPP [2].
During hypokalemia ingress of K+ through Na+K+- ATPase is more than egress through Kir channels and balance between the inward and outward ions can only be reached if resting membrane potential is shifted to depolarized potential [6]. This precludes Na+ channel activation thus resulting in clinical paralysis (Figure 1) [5].
References
-
Vijayakumar A, Ashwath G, Thimmappa D (2014) Thyrotoxic periodic paralysis: clinical challenges. J Thyroid Res pp: 6.
-
Singhai P, Krishnan S, Patil VU (2017) Thyrotoxic Channelopathies. J Assoc Physicians India 65(11): 98-99.
-
Lien YH (2015) Paradoxical Hypokalemia: Where Has All the Potassium Gone? Am J Med 128(3): 217-218.
-
Melo MCC, de Souza JS, Kizys MML, Vidi AC, Dorta HS, et al (2017) Novel linkRNA Susceptibility Gene and its Role in Etiopathogenesis of Thyrotoxic Periodic Paralysis. J Endocr Soc 1(7): 809-815.
-
Falhammar H, Thorén M, Calissendorff J (2013) Thyrotoxic Periodic Paralysis: Clinical and Molecular Aspects. Endocrine 43(2): 272-284.
-
Cheng CJ, Kuo E, Huang CL (2013) Extracellular Potassium Homeostasis: Insights from Hypokalemic Periodic Paralysis. Semin Nephrol 33(3): 237-247.
-
Cannon SC (2010) Voltage-sensor mutations in channelopathies of skeletal muscle. J Physiol 588(11): 1887-1895.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty